Clinical History
A 48-year-old female patient was referred to the orthopaedic department of our institution for painful hip joints. The patient underwent radiography, CT and MRI of the hips.
Imaging Findings
A 48-year-old female patient was referred to the orthopaedic department of our institution for painful hip joints.
The patient had a medical history of congenital subluxation of both hip joints and had difficulty in walking and hip joint mobility.
We performed radiography and CT scan of the hips which revealed left and to a lower degree right congenital hip subluxation with concomitant osteoarthritic lesions of the femoral head, the trochanters and the acetabulum. These lesions included osteophytes and joint space narrowing. The left femoral bone was found in external location and abduction,characteristic for congenital hip subluxation.
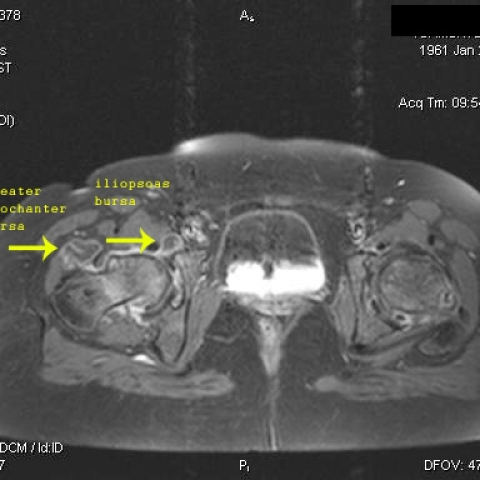
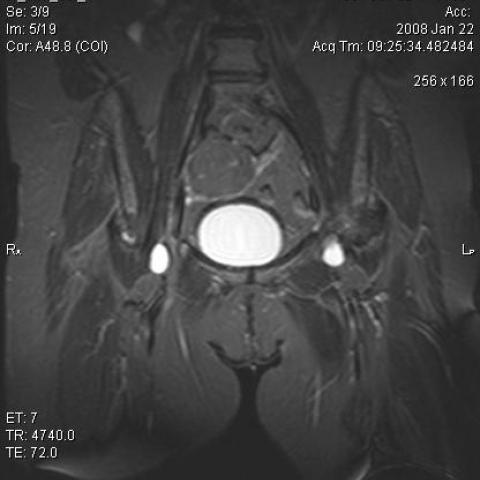
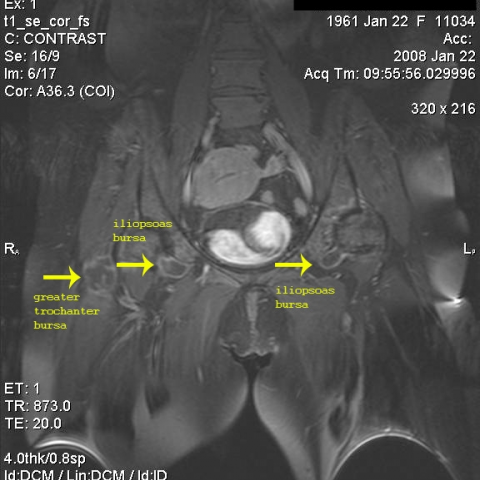
MRI scan confirmed the aforementioned findings and in addition depicted extensive bursitis of both hip joints with enhancement of the bursal walls after contrast medium administration.
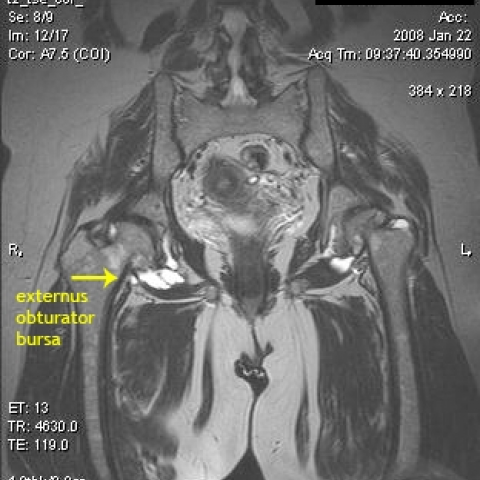
We found extensive fluid collections inside the following major bursae bilaterally:
1) iliopsoas bursa with the characteristic « tear drop» appearance.
2) greater trochanteric bursa. .
3) obturator externus bursa.
These fluid collections were hyperintense on T2W1 and hypointense on T1W1 images.
Discussion
Studies have shown that up to 21 bursae can be found in the hip region with variable extent and prevalence. The 2 major bursae are iliopsoas bursa and greater trochanteric bursa. The iliopsoas bursa, the largest bursa in the body, lies between the iliopsoas tendon and the lesser trochanter, extending upward into the iliac fossa beneath the iliacus muscle and may approach 3-7cm in length and 2-4 cm in width. Three constant bursae surround the greater trochanter(two major and a minor). the two major bursae include the subgluteus medius and the subgluteus maximus bursa. The gluteus medius is situated posterior and superior to the proximal edge of the greater trochanter. The subgluteus maximus is lateral to the greater trochanter. It is almond shaped, 4 to 6 cm in length and 2-4 cm in width. The minor bursa is the gluteus minimus bursa, which lies above and slightly anterior to the proximal surface of the greater trochanter.
Bursitis is inflammation of a bursa caused by repetitive use, trauma, infection, or systemic inflammatory disease. Bursae are flattened sacs that serve as a protective buffer between bones and overlapping muscles (deep bursae) or between bones and tendons/skin (superficial bursae).Iliopsoas bursitis is often associated with hip pathology (eg, rheumatoid arthritis, osteoarthritis) or recreational injury (eg, running). Pain from iliopsoas bursitis radiates down the anteromedial side of the thigh to the knee and is increased on extension, adduction, and internal rotation of the hip.
Patients with trochanteric bursitis are predominately women (male-to-female ratio of 2-4:1) in their fourth to sixth decade of life . The disease is also associated with rheumatoid arthritis of the hips, osteoarthritis of the hips, lumbosacral disease, and leg-length discrepancies. Patients experience chronic, intermittent, aching pain over the lateral hip. In 40% of cases, this radiates down to the lateral thigh. Walking or lying on the affected side exacerbates the pain. In the seated position, local tenderness is present over the greater trochanter or more posteriorly for deep bursa. Pain can be reproduced by hip adduction (superficial bursitis) or resisted active abduction (deep bursitis).
The obturator externus bursa has been described in anatomy textbooks as a potential bursa between the tendon of the obturator externus muscle and the posterior hip capsule. This bursa lies between the ischiofemoral capsular ligaments and the tendon of the obturator externus muscle as it spirals, posterior to the femoral neck, toward its insertion into the trochanteric fossa.
Diagnosing bursitis is based mainly on clinical findings. Normally, bursae are in a collapsed state, and are only distended and visualized by MRI when they are inflamed or infected. The fluid collections inside the inflamed bursae appear hyperintense on T2W1 and hypointense on T1W1 images. After contrast administration ,enhancement of the bursal walls is observed on T1W1 images.
Differential Diagnosis List
Bilateral bursitis at the major bursae of the hip joints
Final Diagnosis
Bilateral bursitis at the major bursae of the hip joints