Clinical History
A 23-year-old woman presenting with fever and a left flank pain was admitted to our Hospital. The patient did not suffer from diabetes or lithiasis or renal insufficiency. Urine culture was negative.
Imaging Findings
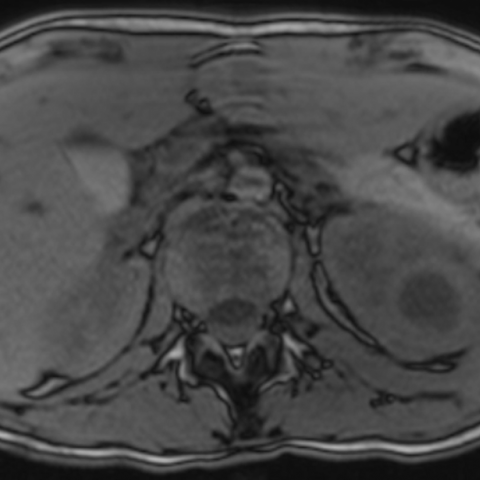
An abdominal US detected a hypoechoic, encapsulated round mass at the upper pole of the left kidney, measuring 2.5 cm in diameter (Fig. 1). Because of her young age, the patient was then referred for a MR investigation with a 3T magnet. The lesion was hypointense on T1-weighted MRI and hyperintense on T2-weighted without and with fat saturation MRI, whereas the pseudocapsule was isointense to the renal cortex and hypointense, respectively (Fig. 2). The mass showed restricted water diffusion on DWMRI; the mean ADC value of the lesion was 950. DWMRI also demonstrated a perilesional water diffusion restriction (Fig. 3). The lesion did not enhanced on dynamic contrast-enhanced MRI, whereas the pseudocapsule progressively enhanced in the late venous phase (Fig. 4). Similar features were also observed into the ipsilateral perinephric space and the quadratus lomborum muscle (Fig. 5).
Discussion
Patients with urinary tract infection non responder to medical therapy as well as immunocompromised or diabetics patients should undergo early radiological investigations to assess underlying anatomical abnormalities and to depict complications [1]. Despite its ability in detecting renal and perirenal pathologies, US, usually firstly performed in these patients, is less sensitive than CT in detecting complications of the upper urinary tract infection. In these instances CT is considered the golden standard because of its superiority in diagnosis, staging and follow-up patients; an accurate CT technique, which should include non-enhanced and multiphasic dynamic scans, is necessary to achieve a correct diagnosis [1]. Unfortunately allergy and side effects to the iodinated contrast medium can contraindicate CT; moreover radiation exposure from a multiphasic CT investigation can be a further drawback, especially in young patients [1]. In these cases MRI can substitute CT, which findings are similar on contrast enhanced imaging; however radiologists should keep in mind that gas bubbles and stones can be difficult to identify on MRI [1, 2]. Abscess has low signal on T1-weighted MRI and a high signal on T2-weighted MRI; a fluid-fluid level can be sometimes detected. The pseudocapsule, typical of a mature abscess, characteristically enhances in the late venous and excretory phases [1]. As observed in dynamic CT, the abscess can be surrounded by a halo of decreased enhancement, which likely represents an infected but non-necrotic perilesional parenchyma [2, 3]. Extrarenal spread of the abscess can also easily be demonstrated with MRI due to multiplanar imaging [4]. DWMRI is an attractive technique in diagnosing abdominal abscess and can improve the sensitivity in T2-weighted and contrast enhanced MRI [5]. Because of the high content of inflammatory cells, bacteria, proteins and debris water diffusion is restricted in abdominal abscesses, resembling DWMRI features of brain abscess; similarly the mean apparent diffusion co-efficient (ADC) is lower than in non-infected fluid collection and necrotic tumours [5].
Differential Diagnosis List
Renal abscess extending
Cyst
Infected cyst
Cystic neoplasm
Hemorrhagic cyst
Focal xanthogranulomatous pyelonephritis