Clinical History
A 35-year-old primigravid woman was admitted in the 30th week of gestation with sudden epigastric pain. Clinical examination revealed hypertension (150/100 mmHg) and abdominal tenderness without peritoneal reaction. Laboratory evaluation depicted Hb 7,9 g/dl, leucocytosis (21 x109/L), neutrophilia, high serum ALT /AST, hypoalbuminaemia,proteinuria and normal bilirubin and platelet count.
Imaging Findings
Abdominal ultrasound (US) showed moderate hepatomegaly with a huge heterogeneous collection with thin septa and non-pure echogenic content, along the anterior and lateral border of the right hepatic lobe, measuring about 11.5 x 6.3 x 8.2 cm (Fig 1). The gallbladder, although non-distended, presented moderate parietal thickening and echogenic bile. There was a small quantity of intra-peritoneal fluid and a small right pleural effusion (Fig 1:arrows).
Based on the hypothesis of hepatic hematoma in a moderate pre-eclampsia context, it was decided to terminate pregnancy by caesarean section. Surgical exploration corroborated the hematic nature and integrity of the collection, without signs of rupture.
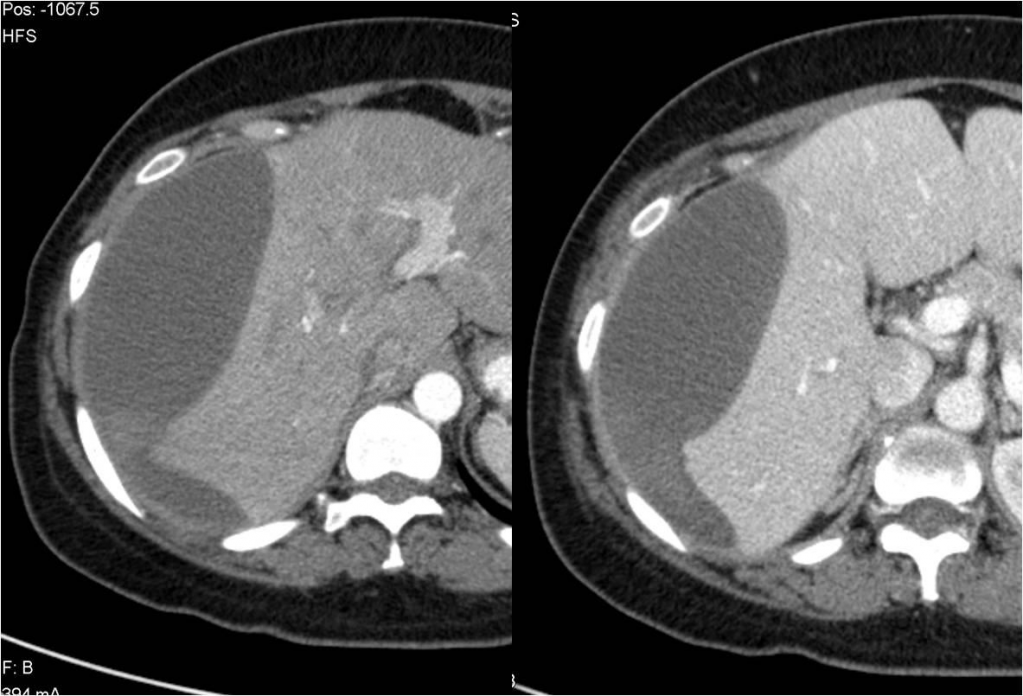
Contrast-enhanced abdominal computed tomography (CT) performed after delivery revealed signs of recent hemorrhage within a subcapsular hematoma (Fig 2 & 3). The patient evolved clinically well and CT 3 months later showed absence of recent hemorrhage or any underlying liver lesion.
Discussion
Sub-capsular hepatic hematoma during pregnancy is rare, with a reported incidence that varies from 1 in 40, 000 to 1 in 250, 000 deliveries [1]. It usually complicates pre-eclampsia or the HELLP syndrome (HELLP = haemolysis, elevated liver enzymes, low platelet), with few published cases in the absence of hypertension [2]. Marked elevation of serum aminotransferases are not typical of uncomplicated HELLP syndrome, and when they occur, the possibility of hepatic infarction and subcapsular hematoma of the liver must be considered [3] . The differential diagnosis includes acute fatty liver of pregnancy, abruption placentae with disseminated intravascular coagulation, acute cholecystitis, viral hepatitis and thrombotic thrombocytopenia purpura. Most patients with hepatic hematoma are seen in the late second or third trimester of pregnancy, although cases have been reported in the immediate postpartum period [4].
The aetiology of sub-capsular hemorrhage in patients with hypertensive disorders of pregnancy is probably due to fibrin thrombi in hepatic arterioles and sinusoids with periportal hemorrhagic necrosis [5].
Ultrasonography remains the first imaging modality for the diagnosis of this complication and 3D ultrasonography is rapidly gaining popularity as
it offers several distinct advantages over conventional ultrasound [6]. CT and MR imaging may also play an important role both in the diagnosis and follow-up.
The management of contained hematoma is usually conservative [2], with volume replacement and blood transfusion, as needed. Surgery is reserved for those with expanding and/or rupture of the haematoma. Surgical options include packing of the bleeding surface with absorbable sponge, suture of omental patch or surgical mesh, hepatic resection or even transplantation in case of intractable hemorrhage[3]. Rarely, percutaneous embolisation of the hepatic arteries and Argon beam coagulator has been reported [1].
Differential Diagnosis List
Hepatic subcapsular haematoma in pre-eclampsia
Hepatic abcess
Acute cholecystitis
Final Diagnosis
Hepatic subcapsular haematoma in pre-eclampsia