


Figure 1
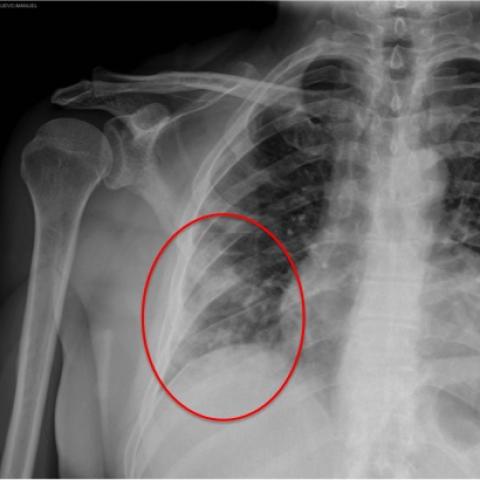
Oblique chest radiography: small ground-glass opacities (circle) in the right lung base not visible on previous imaging studies.
Chest imaging
Case TypeClinical Cases
Authors
Paula Concejo Iglesias
62 years, male
A 62-year-old male patient with chemotherapy treatment under treatment with chemotherapy due to a recently diagnosed rectum adenocarcinoma.
He arrived because of syncope and traumatism in the right hemithorax. The patient did not display any did not refer other symptoms.
New consolidations in the right hemithorax were evidenced found in chest radiography and asymptomatic COVID-19 was suggested and confirmed by polymerase chain reaction (PCR).
Anteroposterior and oblique radiographs were performed to evaluate the ribs, which were normal. Incidentally, evidence of small opacities were found As an incidental finding small opacities were evidenced in the right lung base. A chest NECT was performed, due to a In suspicion of COVID-19 infection, a chest NECT was performed.
On CT, peripheral ground-glass opacities affecting all lobes of the right lung were confirmed, the same side where the patient had the traumatism without compatible symptoms of chest infection.
A global health emergency was declared in January 2020 by the World Health Organization (WHO), due to a secondary to a coronavirus disease (COVID-19) [1- 5] caused by a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1-4, 6] which may result in a life-threatening and rapidly progressive viral pneumonia (2). SARS-CoV-2 belongs to the family Coronaviridae [1, 2, 5] as well as the viruses that cause severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) [1, 3, 5].
The infection began in China and rapidly spread worldwide [1, 2, 4- 6]. Rapid and accurate diagnosis is mandatory in order to prevent human-to-human transmission [1, 5, 6] as well as with the isolation of those patients infected patients [1, 6] coupled with a good patient management and for the best management for them [1]. Transmission can occur during the incubation period and in asymptomatic patients [5]. Children are 's population is less affected than adults and when it occurs, they present mild symptoms [1].
An alteration of the angiotensin-converting enzyme II inducing diffuse alveolar damage by the virus has been postulated [1]. It is usually presented with fever, dry cough, dyspnea, respiratory distress, and muscle pain. [3-5].
Reverse transcription-polymerase chain reaction (RT-PCR) [4, 6] or gene sequencing of the virus [6] of the nasopharyngeal aspiration are the standard diagnostic method [4, 6] although there are patients with false-negative results [1, 2, 4, 6], especially in early stages [1, 2]. Chest CT may be an important tool for prompt diagnoses and a follow-up of infected patients by SARS-CoV-2 [1-3, 5, 6]. Imaging findings can be seen before symptoms or positive laboratory test results [1].
75% of imaging studies reveal bilateral involvement [5]. The most frequent imaging findings are ground-glass opacity and consolidation in peripheral [1- 4, 6] and posterior localization. These involve the involving lower and middle areas [1- 3], that increase in size and number as the disease progresses when disease progress with the affection of the upper areas of the lung [1, 2], which has been seen in 75% of patients [1]. Although less frequently, vascular enlargement, interlobular septal thickening, air bronchogram sign, air trapping, reversed halo sign, pulmonary nodules with halo sign [1, 2], crazy paving [2-4], bronchiectasias and pleural thickening [2] can also be seen.
Some patients may develop irreversible injury of the lung parenchyma with fibrosis [1, 3].
In summary, chest CT is a widely available and rapid diagnostic tool for COVID-19 useful in differentiating infected patients even before laboratory tests.
Although chest CT is not specific for a diagnosis of COVID-19 pneumonia, it may be helpful in confirming typical findings in patients at risk for COVID infection with or without clinical symptoms in the absence of a positive PCR test. Furthermore, if typical findings are detected incidentally, as in our case, radiologists should alert referring physicians to the possibility of COVID-19 infection.
[1] Li, Y., & Xia, L. (2020). Coronavirus Disease 2019 (COVID-19): Role of chest CT in diagnosis and management. American Journal of Roentgenology, 1-7. DOI: 10.2214/AJR.20.22954
[2] Salehi, S., Abedi, A., Balakrishnan, S., & Gholamrezanezhad, A. (2020). Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. American Journal of Roentgenology, 1-7. DOI: 10.2214/AJR.20.23034
[3] Chung, M., Bernheim, A., Mei, X., Zhang, N., Huang, M., Zeng, X., ... & Jacobi, A. (2020). CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology, 200230. doi.org/10.1148/radiol.2020200230
[4] Bai, H. X., Hsieh, B., Xiong, Z., Halsey, K., Choi, J. W., Tran, T. M. L., ... & Jiang, X. L. (2020). Performance of radiologists in differentiating COVID-19 from viral pneumonia on chest CT. Radiology, 200823. doi.org/10.1148/radiol.2020200823
[5] Kooraki, S., Hosseiny, M., Myers, L., & Gholamrezanezhad, A. (2020). Coronavirus outbreak: what the department of radiology should know. Journal of the American College of Radiology. doi.org/10.1016/j.jacr.2020.02.008
[6] Ai, T., Yang, Z., Hou, H., Zhan, C., Chen, C., Lv, W., ... & Xia, L. (2020). Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology, 200642. doi.org/10.1148/radiol.2020200642
| URL: | https://www.eurorad.org/case/16751 |
| DOI: | 10.35100/eurorad/case.16751 |
| ISSN: | 1563-4086 |
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.











