Figure 1
Sagittal (1a) and coronal (1b) T1-weighted images after gadolinium contrast
Head & neck imaging
Case TypeClinical Cases
Authors
Anca Oprisan, Eduardo Baettig-Arriagada, Ali Boukhoubza, Vicent Belloch-Ripolles, Marialaura Mena-Cavelis, Macarena Barreda-Solana, Miguel Mazón, Fernando Aparici-Robles
48 years, female
A 50-year-old woman with a severe case of depression refers anosmia, bradypsychia, bilateral hearing loss and hypersomnia. The physical examination highlights a mild bilateral exophthalmos, without sings of neurological focality.
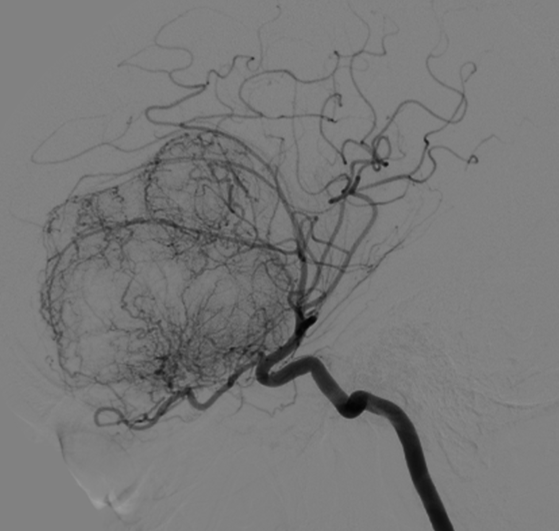
A cerebral MRI is performed identifying a large extra-axial mass with an enostotic spur in the planum sphenoidale (Fig. 1). It encompasses the clinoid processes and extends through the greater sphenoid wings. The mass effect conditions a marked deformity of the anterior portion of the brain, with transtentorial descending herniation and herniation of the third ventricle to the prepontine cistern (Fig. 2). The MRI also illustrated an empty sella, encephalocele of petrosal right apex and marked ectasia of the optic nerve sheaths, with protrusion of the heads in eyeballs (Fig. 2). A homogeneous and intense enhancement is evidenced after the administration of contrast (Fig. 3). All the findings suggest that the lesion corresponds to an olfactory groove meningioma. The study was completed with a cerebral angiography, which revealed the vascularisation of the meningioma by the ophthalmic, anterior cerebral, maxillary and meningeal arteries (Fig. 4).
Meningiomas are usually benign tumours, slow-growing, originating in the meningothelial cells located in the arachnoid membrane. They represent approximately 15% to 20% of intracranial tumours.
Olfactory groove meningiomas represent between 8 and 13% of all intracranial meningiomas [1,2]. They usually occupy the anterior fossa of the skull in the cribriform plate area, and may involve the crista galli, the posterior part of the sphenoid plane. It can extend symmetrically over the midline or laterally. In cases of large tumours, many neurological structures can either be compressed or rejected [2]. The compression of the optic and olfactory nerves, and the chiasm will result in visual and olfactory deficits; while the pressure on the third ventricle can cause hydrocephalus. The tumour usually grows exophytically, even though the implant is in the midline of the anterior fossa, where the dura mater and the underlying bone are thin [3].
The olfactory groove meningiomas grow slowly and in an area of scarce neurological expressivity. However, the diagnostic suspicion often arises from an abrupt clinical manifestation. In these cases, minor symptoms or gradual development that went unnoticed are recognised [3]. The most common clinical presentation is cognitive deterioration, visual impairment, anosmia and headache.
The initial diagnosis of meningioma is achieved by imaging, being the technique of choice MRI. Nonetheless, in order to know the disposition of the paranasal sinuses, identify intratumoral calcifications and erosions or hyperostosis induced by the tumour, a preoperative study with CT is recommended [4]. The final diagnosis is obtained after the histological study.
The olfactory groove meningioma behaves in the images as any other meningioma. In MRI, it is usually isointense with the cerebral cortex in all the sequences, and, after the administration of the contrast, it presents a typical intense enhancement [5]. In contrast-free CT, it usually has a hyperdense appearance, with calcifications in up to a third of cases, and in post-contrast CT it has bright and homogeneous contrast enhancement.
Resorting to the use of a cerebral angiography can help identify the vessels that supply the meningioma, achieving better surgical planning and results [4].
Symptomatic olfactory groove meningiomas should be treated surgically aiming for a radical resection, with the most frequent surgical approaches being the bifrontal, the unilateral subfrontal or the front-lateral [3]. Our patient underwent a resection through the bifrontal approach.
Written informed patient consent for publication has been obtained.
[1] Nakamura M, Struck M, Roser F, Vorkapic P, Samii M (2007) Olfactory groove meningiomas: clinical outcome and recurrence rates after tumor removal through the frontolateral and bifrontal approach. Neurosurgery, 60:844-852 (PMID: 17460519)
[2] García-Navarrete E, Sola RG (2002) Clinical and surgical aspects of meningiomas of the base of the skull. 1. Meningiomas of the anterior fossa. Rev Neurol. 34(6):584-92 (PMID: 12040506)
[3] González-Darder JM, Pesudo-Martínez JV, Bordes-García V, Quilis-Quesada V, Talamantes-Escrivá F, González-López P, Masbout-Kayal G (2011) Olfactory groove meningiomas: Radical microsurgical treatment through the bifrontal approach. Neurocirugía, 22(2):133-139 (PMID: 21597654)
[4] Gelabert-González M, Serramito-García R (2011) Intracranial meningiomas: II. Diagnosis and treatment. Rev Neurol. 53(4):226-232 (PMID: 21780074)
[5] Elster AD, Challa VR, Gilbert TH et-al (1989) Meningiomas: MR and histopathologic features. Radiology.170(3):857-62 (PMID: 2916043)
| URL: | https://www.eurorad.org/case/16533 |
| DOI: | 10.35100/eurorad/case.16533 |
| ISSN: | 1563-4086 |
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.

T1-weighted images without contrast
T1-weighted contrast
Cerebral angiography