Figure 1

Head & neck imaging
Case TypeClinical Cases
Authors
Tarigan Agnes ; Violetta Lenny
21 years, female
A 21 year old female was referred from Ear, Nose and Throat Department with suspicion of base tongue tumor
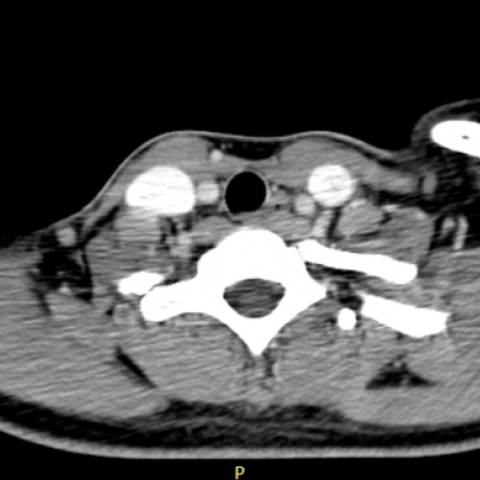
Head and neck CT scan revealed a hyper dense soft tissue lession, solid with numeral small hypodense component, well defined border in foramen caecum of tongue, with enhanced CT Scan there was no significant contrast enhancement (134 HU to 139 HU). The lession slightly protruding to the posterior side caused mild oropharyngeal airway narrowing, still have well defined margin with epiglottis but slightly abutting the epiglottis. US thyroid revealed abscence of thyroid parenchyme in normal anatomical position. US can not revealed any lession in base of tongue.
A suspicion for base tongue tumor was removed and a diagnosed of lingual thyroid was made.
Lingual thyroid is an ectopic thyroid which is an embryological abnormality that results from the failure migration of the thyroid gland from the primitive foregut to the normal thyroid position at the neck.[1] Ectopic Thyroid can occur anywhere such as in the trachea, mediastinum, aortic arch, heart and mediastinum but the most common site is lingual (90%) and can occur at any age from birth to 83 years.[3]
In general, lingual thyroid patient have no symptoms. Symptoms that are often complained by the patient are the mass effect on the base of the tongue which can cause dysphagia, dysphonia and airway obstruction and bleeding.[2] Usually, lingual thyroid is the only thyroid gland so that the patient can develop hypothyroidism.[2-3] This patient was initially suspected for base tongue tumor. The patient didn't complaint other abnormality, no complaint of dysphagia, dyspnoea, hoarseness of voice or any hypothyroid symptom.
On physical examination were found a mass in the base of the tongue, reddish, painless and no bleeding. Laboratory results (T4: 1.29 ng / dl), T3: 1.27 ng / ml), although TSH was mildly elevated (17, 049 uIU / ml), but there were no symptoms associated with abormality thyroid hormone in this patient. On Histopathological examination were found various size of thyroid follicles and no signs of malignancy.
There are no gold standards for lingual thyroid therapy. Surgery is not always needed. Surgery is only done to eliminate symptoms such as airway obstruction. Some suggest complete surgical resection because of concerns about malignant transformation. For asymptomatic and eutiroid cases it is recommended to follow up regularly considering the enlargement of the mass and complications.[4–9] This patient treated with partial resection because the lession slightly protruding to posterior side caused oropharyngeal airway narrowing.
Imaging is important to make a diagnosis and therapy of lingual thyroid. Head and Neck CT Scan can revealed an ectopic thyroid and removed other caused base tongue tumor by the characteristic the lession which identical like thyroid parenchyme. The well defined, smooth contour, homogenous density, prominent enhancement (only occasional case with inhomogenous contrast enhancement) but in abnormal position (foramen caecum of tongue) and abscence of thyroid in normal position.
Written informed patient consent for publication has been obtained.
[1] Guerra G, Cinelli M, Mesolella M, Tafuri D, Rocca A, Amato B, et al (2014) Morphological, diagnostic and surgical features of ectopic thyroid gland: A review of literature. Int J Surg [Internet] Aug;12:S3–11. (PMID: 24887357)
[2] Noussios G, Anagnostis P, Goulis DG, Lappas D, Natsis K (2011) Ectopic thyroid tissue: Anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol 165(3):375–82 (PMID: 21715415)
[3] Yoon JS, Won KC, Cho IH, Lee JT, Lee HW (2007) Clinical Characteristics of Ectopic Thyroid in Korea. Thyroid [Internet]. Nov;17(11):1117–21 (PMID: 17887928)
[4] Douglas PS, Baker AW (1994) Lingual thyroid. Br J Oral Maxillofac Surg [Internet] Apr;32(2):123–4. (PMID: 8199145)
[5] Lianos G, Bali C, Tatsis V, Anastasiadi Z, Lianou E, Papathanasiou V, et al (2013) Ectopic thyroid carcinoma. Case report. Apr;34(4):114–6 (PMID: 23660162)
[6] Toso A, Colombani F, Averono G, Aluffi P, Pia F. (2009) Lingual thyroid causing dysphagia and dyspnoea. Case reports and review of the literature. Acta Otorhinolaryngol Ital Aug;29(4):213–7 (PMID: 20161880)
[7] Chawla M, Kumar R, Malhotra A. (2007) Dual Ectopic Thyroid: Case Series and Review of the Literature. Clin Nucl Med Jan;32(1):1–5 (PMID: 17179793)
[8] Bersaneti JA, Silva RDP, Ramos RRN, de Medeiros Matsushita M, Souto LRM (2011) Ectopic Thyroid Presenting as a Submandibular Mass. Head Neck Pathol Mar 21;5(1):63–6 (PMID: 20857245)
[9] Shah BC, Ravichand CS, Juluri S, Agarwal A, Pramesh CS, Mistry RC (2007) Ectopic thyroid cancer. 1. Guerra G, Cinelli M, Mesolella M, Tafuri D, Rocca A, Amato B, et al. Morphological, diagnostic and surgical features of ectopic thyroid gland: A review of literature. Int J Surg [Internet]. 2014 Aug;12:S3–11. Available from: http://dx.doi.org/10.1016/ Apr;13(2):122–4 (PMID: 17505421)
| URL: | https://www.eurorad.org/case/16341 |
| DOI: | 10.1594/EURORAD/CASE.16341 |
| ISSN: | 1563-4086 |
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.