Figure 1
Coronary angiogram

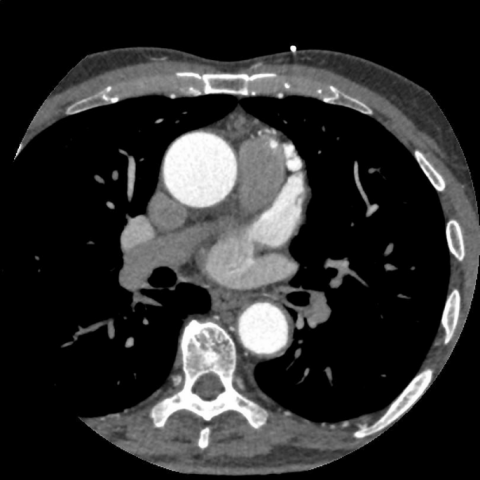
Invasive coronary angiogram where the presence of a coronary-to-pulmonary artery fistula with a single prominent tract, originating from the proximal LAD can be identified.

Invasive coronary angiogram where the presence of a coronary-to-pulmonary artery fistula with a single prominent tract, originating from the proximal LAD can be identified

Invasive coronary angiogram where the presence of a coronary-to-pulmonary artery fistula with a single prominent tract, originating from the proximal LAD can be identified.

Invasive coronary angiogram where the presence of a coronary-to-pulmonary artery fistula with a single prominent tract, originating from the proximal LAD can be identified (areas marked in red).