Figure 1
T2W/FLAIR images of dysplastic gangliocytoma
Neuroradiology
Case TypeClinical Cases
AuthorsKaterina Manavi, Galateia Skouroumouni, Filippos Sarafis, Giannis Petmezaris, Eliza Stavride, Ioannis Tsitouridis
77 years, female
[1] Hariri OR, Khachekian A, Muilli D, et al. (2013) Acute-onset cerebellar symptoms in Lhermitte-Duclos disease: case report. Cerebellum 12(1):127-30 (PMID: 22692559)
[2] Ozeren E, Gurses L, Mehmet S, Er U, Önder E, Arıkök AT (2014) L'hermitte-Duclos disease in an elderly patient: a case report and review of the review of the literature. Asian J Neurosurg 9(4):246 (PMID: 25685239)
[3] Yağci-Küpeli B, Oguz KK, Bilen MA, Yalçin B, Akalan N, Büyükpamukçu M. (2010) An unusual cause of posterior fossa mass: Lhermitte-Duclos disease. J Neurol Sci 290(1-2):138-41 (PMID: 20060133)
[4] Williams LG, Brimage P, Lechner C, Taylor RL, Masters L, Welgampola MS (2014) Lhermitte-Duclos disease presenting with atypical positional nystagmus. J Clin Neurosci 21(9):1647-9 (PMID: 24842320)
[5] Inoue T, Nishimura S, Hayashi N, Numagami Y, Kaimori M, Nishijima M (2007) Ectopic recurrence of dysplastic gangliocytoma of the cerebellum (Lhermitte-Duclos disease): a case report. Brain Tumor Pathol 24(1):25-9 (PMID: 18095141)
[6] Anik Y, Anik I, Koc K, Inan N, Akansel G, Demirci A (2007) MR Spectroscopy findings in Lhermitte-Duclos disease. A case report. Neuroradiol J 20(3):278-81 (PMID: 24299666)
[7] Sen KK, Gunasekaran K, Kanagaraj V (2013) Imaging in Lhermitte: Duclos disease. South Asian J Cancer 2(3):131 (PMID: 24455585)
[8] . Yang MS, Kim CH, Cheong JH, Kim JM (2012) Lhermitte-Duclos disease presenting with hydrocephalus. Acta Neurochir Suppl 113:161-5 (PMID: 22116444)
[9] Giorgianni A, Pellegrino C, De Benedictis A, et al. (2013) Lhermitte-Duclos disease. A case report. Neuroradiol J 26(6):655-60 (PMID: 24355184)
| URL: | https://www.eurorad.org/case/14955 |
| DOI: | 10.1594/EURORAD/CASE.14955 |
| ISSN: | 1563-4086 |
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.

T2W/FLAIR images of dysplastic gangliocytoma
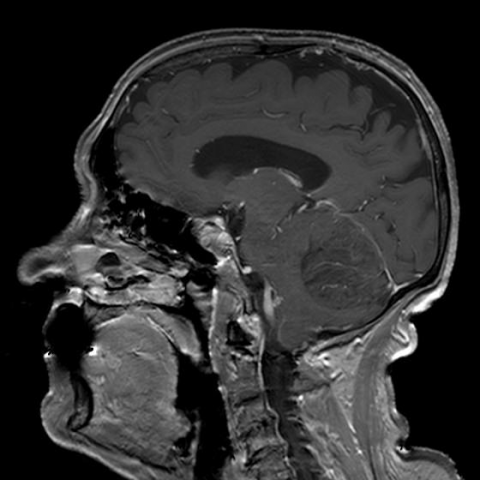
Gadolinium-enhanced T1W images of dysplastic gangliocytoma
DWI/ADC images of dysplastic gangliocytoma