Clinical History
Preterm infant of 36 gestational weeks with respiratory distress and suspected sacral agenesis. X-ray of the abdomen was taken for evaluation of lungs and bowel gas to start feeding.
Imaging Findings
Plain film of the abdomen shows osseous structures demonstrating 13 pairs of ribs; in addition, no lumbar or sacral vertebral bodies are present, and there is overlapping of the bilateral iliac wings (Fig. 1)
Ultrasound of the spinal canal shows the conus medullaris extending to the level of T12. Inferior to this level no vertebral bodies or spinal canal is identified (Fig. 2)
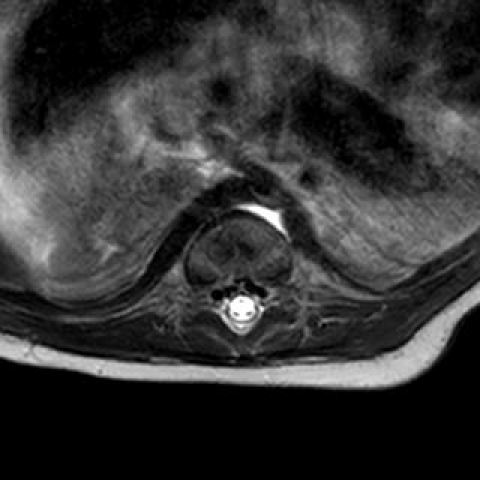
MRI shows 7 cervical and 12 thoracic segments. There is not formation of the spinal segments below a hypoplastic/dysplastic L1 segment. There is abrupt termination of the central spinal canal at the malformed L1 segment with the normal thecal sac terminating approximately at the T11-T12 disc. There is marked blunting of the conus which terminates at the T10 level. No cord signal abnormality is identified.
Discussion
Caudal regression syndrome (CRS), also known as caudal agenesis, results from abnormal development of the caudal aspect of the spinal cord and vertebral column due to an earlier abnormality of gastrulation [1]. Its precise aetiology is not known but toxic, ischaemic or infectious aetiologies before the 4th week of gestation are thought to be associated with this syndrome.
CRS is divided into two types according to Andrea Rossi and Paolo Tortori-Donati. [1].
In type 1 the conus medullaris is high and abrupt, with associated vertebral aplasia in several grades of coccygeal, sacral, lumbar, and lower thoracic vertebrae.
In type 2 the conus medullaris is low and tethered by a thickened filum terminale, intraspinal lipoma, terminal myelocystocele, or lipomyelomeningocele.
There is an association with maternal diabetes, and adequate control of diabetes before conception and during the first few weeks of gestation is associated with decreased incidence of this syndrome [2]. Clinically, patients present with a wide spectrum of symptoms ranging from mild to severe motor and sensory deficits in the lower extremities, neurogenic bladder, faecal incontinence and vesicoureteric reflux. Progressive neurological symptoms suggest tethering of the spinal cord located below the L1 level [2].
Diagnosis can usually be made in the 2nd or 3rd trimester with prenatal ultrasound, which demonstrates sacrococcygeal dysgenesis. Ultrasound is also helpful in evaluating other associated anomalies such as renal anomalies including agenesis, cystic dysplasia and caliectasis, and gastrointestinal anomalies such as duodenal atresia [2]. Fetal MRI can also be used to make the diagnosis in difficult cases [2]. Due to incomplete penetration of the ultrasound caused by ossified vertebrae, MRI is the imaging modality of choice for the diagnosis of any vertebral and spinal cord pathologies in postnatal state [3]
MR neurography is a helpful tool in the evaluation of the nerve root abnormalities [3].
Prenatal diagnosis is important so that appropriate patient counselling can be provided and postnatal interventions performed.
The main differential diagnosis of caudal regression syndrome is sirenomelia that is characterised by a more pronounced caudal dysgenesis with fused lower extremities. The presence of abnormally small abdominal aorta, and renal agenesis or severe dysgenesis with severe oligohydramnios and pulmonary hypoplasia makes it more severe and fatal [4].
The treatment depends upon clinical symptoms, including the degree of neurological deficits. The main goals of treatment include maintaining and improving renal, cardiac, pulmonary and GI function, preventing renal infection and achieving continence [4].
Differential Diagnosis List
Caudal regression syndrome
Sirenomelia
Meningocele
Lipomyelomeningocele
Sacrococcygeal teratoma
Final Diagnosis
Caudal regression syndrome