Clinical History
A 56-year-old woman presented with progressive intermittent claudication of the left lower extremity.
Imaging Findings
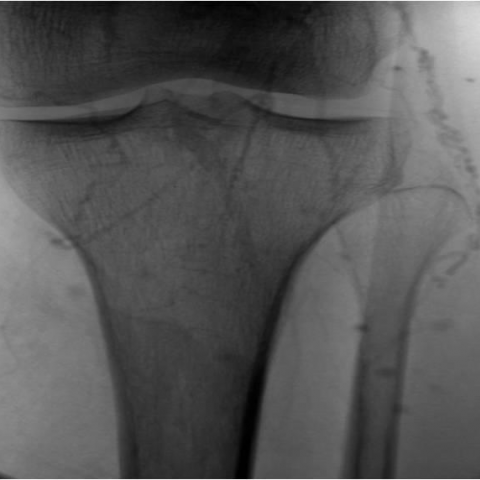
Multislice spiral CT angiography (CTA) showed an abrupt interruption of the lower third of the superficial left femoral artery and the proximal part of the left popliteal artery. Arterial collateral vessels bypassing the occluded segment, supplied the popliteal artery in the popliteal fossa. There were no atherosclerotic changes of the arterial wall. The occluded vessel was abnormally located, medially to the inner head of the left gastrocnemius muscle that was more laterally inserted and more hypertrophied compared to the right side. The non-opacified segment of the popliteal artery was substantially narrowed by the external muscular hypertrophy. The popliteal vein coursed normally between the heads of the gastrocnemius muscle, separately from the artery.
Discussion
Popliteal artery entrapment syndrome (PAES) is an important, yet unusual cause of vascular claudication. PAES is caused by an aberrant anatomic relationship between the popliteal artery and the neighbouring muscles and tendinous structures [1]. Embryologically, the popliteal fossa is the “anatomical arena” between the muscles that migrate and attach and the arteries that fuse and form [2]. The migration of the medial head of the gastrocnemius muscle (MHGM) and the formation of the popliteal artery occur simultaneously. If the arterial development precedes, it may lead to arrest of the migration of the MHGM [2]. Aberrant attachment of the MHGM to the lateral aspect of the medial femoral condyle results in entrapment and compression of the popliteal artery [2] (Fig. 1a, 1b). Repetitive vascular wall microtrauma progresses to fibrosis and permanent narrowing of the vessel, predisposing to thrombosis. In the latter case patients may even present with acute limb threatening ischaemia [3]. Precocious local atherosclerotic changes, embolic episodes, post-stenotic ectasia and even aneurysm formation have also been reported in the setting of PAES [3]. Clinical suspicion of PAES requires the realization of provocative tests that reproduce the symptoms and by means of duplex ultrasonography induce pathologic monophasic waveforms or absence of flow [4]. Digital subtraction angiography (DSA) demonstrates the medial deviation of the artery, the arterial narrowing or occlusion and the collateral circuit (Fig. 2a, b). Tomographic methods such as CTA and MR provide additional anatomical information about the muscles in the popliteal fossa [3] (Fig. 1, 3). The treatment of claudication involves a surgical approach since the resection of the aberrant muscle offers a direct release of the artery. If the vessel is totally occluded an autologous venous graft may replace the segment [3].
PAES should be included in the differential diagnosis of vascular claudication in the young and non-atherosclerotic population and CTA findings may help substantially to form the diagnosis.
Differential Diagnosis List
Popliteal artery entrapment syndrome
Cystic adventitial disease
Fibromuscular dysplasia
Buerger’s disease
Vasculitis
Final Diagnosis
Popliteal artery entrapment syndrome