



Figure 1
Initial, presurgical contrast-enhanced CT (MRI unavailable at another facility)

Multiplanar post-contrast images (a...c) showed uterine body with well-demarcated, mildly heterogeneous hypointense endometrial mass (arrowheads), measuring approximately 3x2.5x1.5 cm, which did not appear to involve the cervix. No ascites and lymphadenopathies.

Multiplanar post-contrast images (a...c) showed uterine body with well-demarcated, mildly heterogeneous hypointense endometrial mass (arrowheads), measuring approximately 3x2.5x1.5 cm, which did not extend beyond the uterus. No adnexal enlargement and lymphadenopathies.

Multiplanar post-contrast images (a...c) showed uterine body with well-demarcated, mildly heterogeneous hypointense endometrial mass (arrowheads), which invaded over 50% of myometrium but not full-thickness or beyond the uterus. No adnexal enlargement and lymphadenopathies.

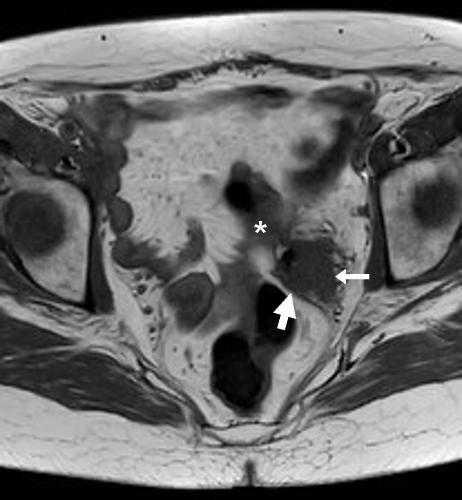
Oblique-axial image from additional excretory-phase CT acquisition after colonic water enema confirmed hypointense endometrial mass (arrowheads) invading over 50% of myometrium but not full-thickness or beyond the uterus.













![[18F]-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET/CT)](/sites/default/files/styles/figure_image_teaser_large/public/figure_image/2018-08/0000014476/000019.jpg?itok=gNVH1MVZ)
![[18F]-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET/CT)](/sites/default/files/styles/figure_image_teaser_large/public/figure_image/2018-08/0000014476/000020.jpg?itok=KDleMyHz)






















![[18F]-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET/CT)](/sites/default/files/styles/figure_image/public/figure_image/2018-08/0000014476/000019.jpg?itok=7ymd80ye)
![[18F]-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET/CT)](/sites/default/files/styles/figure_image/public/figure_image/2018-08/0000014476/000020.jpg?itok=DpUwUg6Y)





