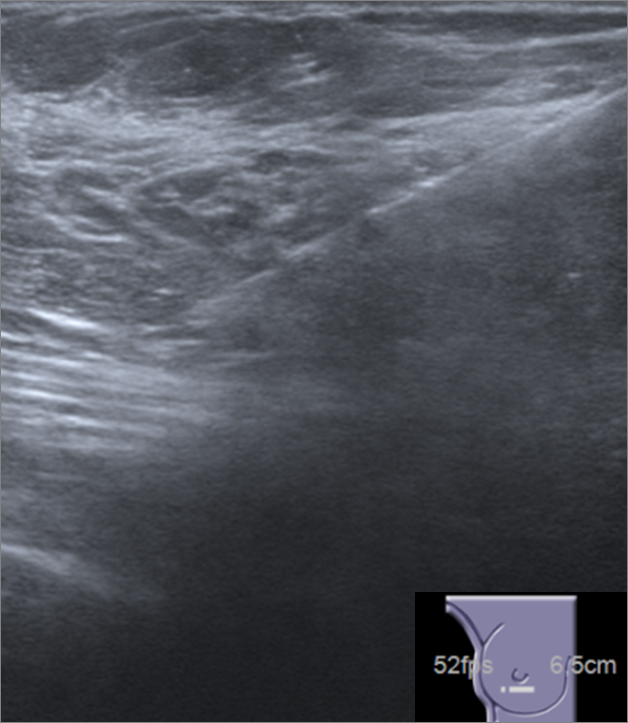
The patient had a history of a treated invasive ductal carcinoma of the left breast in 1992 (stage IA, G1, with clear surgical margins). Simultaneously, in the right breast, a pseudonodular area of dense parenchyma with ductal ectasia, which clinically corresponded to a relatively central, nontender, palpable mass, was characterized as adenosis with core needle biopsy. Since there was an agreement between pathological findings and benign imaging appearance, the patient remained in clinical and mammographic follow-up.
In 2015, our patient presented a new nodular image in the left breast diagnosed at biopsy as a multifocal invasive carcinoma. By the same time, right axillary lymphadenopathies were diagnosed as metastasis of carcinoma. Contralateral location raised the suspicion to another occult malignancy. The increased enhancement pattern at MRI directed the attention to the known right breast lesion, until then considered benign. Core needle biopsy was performed in the right lesion, but the result of adenosis and apocrine metaplasia was not considered tranquilizing in the current clinical setting. Then, vacuum-assisted core biopsy was performed, with the diagnosis of adenomyoepithelioma.
Adenomyoepithelioma of the breast is a rare tumour that belongs to the group of myoepithelial lesions. Most cases are benign, but malignant degeneration is possible. [1]
Histologically, these lesions are characterized by proliferation of epithelial and myoepithelial cells. Some reports describe adenosis as a possible precursor of adenomyoepithelioma. [2, 3]
The imaging features of adenomyoepithelioma are not well established. Most reports describe it as a nodular lesion. Mammographic and ultrasound characteristics, although not specific, can point to the benign or malignant nature of an adenomyoepithelioma. [1, 3]
Our case proved to be an uncommon imaging presentation of an adenomyoepithelioma, as a pseudonodular mammographic lesion. The subtle features and stability of the lesion are in accordance with its benign nature. The clinical and epidemiological features were also compatible with the final diagnosis.
After the diagnosis of a benign adenomyoepithelioma, total excision with a margin of uninvolved tissue is recommended to prevent malignant transformation and local recurrence. [3]
The patient was submitted to a right breast lumpectomy (that confirmed the diagnosis of benign adenomyoepithelioma), besides left mastectomy and right axillary lymphadenectomy to the malignant disease (left multifocal invasive carcinoma NOS, stage IIIC, G2, ER-100%, PR-5%, HER2 negative, Ki67-20%).
Metastasis can occur in malignant adenomyoepithelioma and appear to be haematogenous rather than lymphatic. [3]
Due to the presence of a benign adenomyoepithelioma and no evidence of other malignancies, it was assumed that the right metastatic lymphadenopathies had their origin in the contralateral malignant tumour.