Clinical History
A previously healthy 28 year-old male, from Guinea Bissau, who had lived in Europe for 4 years, presented to the emergency department with fever, dry cough, dyspnoea and weight loss (15kg in 3 months). Physical examination revealed fever (38.2ºC) and reduced respiratory sounds in the left hemithorax. HIV and HBV infections were detected.
Imaging Findings
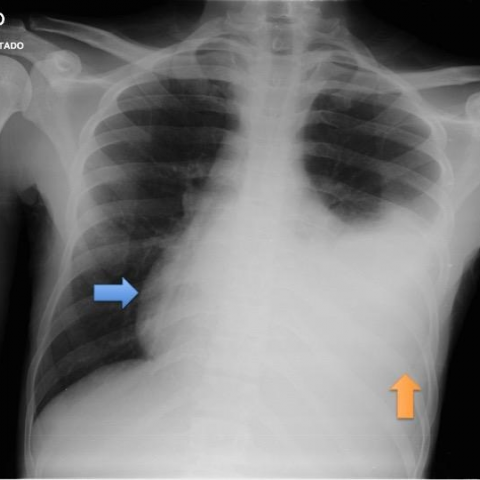
- Chest X-Ray: Cardiac silhouette enlargement and opacification of the lower half of the left hemithorax
- Chest Ultrasound and Echocardiography: Pleural effusion with echoes and pericardial thickening as well as complex pericardial effusion with echoes and septa (images not available)
- Chest CT: Necrotic mediastinal lymph nodes; large pericardial effusion with septa and irregular thickening of the pericardium; large pleural effusion with nodular pleural thickening;random pulmonary micronodules
- Cardiac MRI: Necrotic mediastinal lymph nodes; large pleural effusion; large pericardial effusion with septa and irregular thickening of the pericardium; signs of constrictive pericarditis
Discussion
Background
- Tuberculous pericarditis, caused by Mycobacterium tuberculosis, is rare in developed countries, but is an important aetiology of pericarditis in Africa, owing to the HIV epidemic.
- Pericardial involvement comes from lymphatic spread of M.tuberculosis from peribronchial, peritracheal, or mediastinal lymph nodes or by hematogenous spread from primary tuberculous infection [1].
Clinical Perspective
- Tuberculous pericarditis presents clinically in 3 forms: pericardial effusion, constrictive pericarditis or a combination of both.
- Tuberculous pericardial effusion presents with nonspecific symptoms, such as fever, night sweats, fatigue, and weight loss. Chest pain, cough, and breathlessness are common.
- Patients with constrictive pericarditis present with symptoms of heart failure (dyspnoea, orthopnea, fatigability) and may have liver enlargement and ascites.
- Pericardiocentesis is recommended in all patients in whom TB is suspected [1].
Imaging Perspective
- Chest radiograph may show an enlarged cardiac shadow (>90%), active pulmonary TB features (30%) and pleural effusion (40-60%).
- Transthoracic echocardiography is the first-line technique for pericardial disease and to guide pericardiocentesis. Effusion with fibrinous strands is typical but not specific [1].
- Chest CT and MRI enable detection of pericardial effusion and thickening of the pericardium, while showing enlarged mediastinal lymph nodes, and parenchymal or pleural abnormalities [1]. CT is the best modality for pericardial calcifications [2, 3]. Calcification is a nonspecific response to chronic inflammation, not a definite sign of tuberculous aetiology [3].
- The diagnosis of constrictive pericarditis is aided by CT and MR. The typical appearance is thickening of the pericardium +/- calcifications (>4mm); constrictive symptoms are required for diagnosis. Other imaging findings include tubular-shape of the right ventricle, atrial enlargement, dilatation of the IVC, pleural effusion and ascites [2, 3].
- Cardiac MRI was performed to exclude other causes of right heart failure and coexistent restrictive cardiomyopathy. It did not bring any additional information, besides confirming the findings.
- A definite diagnosis requires demonstration of tubercle bacilli in pericardial fluid or histologic section of the pericardium. A probable diagnosis is based on unexplained pericarditis in a patient with tuberculosis elsewhere, a lymphocytic pericardial exudate with elevated ADA activity or good response to a trial of antituberculosis chemotherapy [4].
Outcome
- Treated with antituberculosis chemotherapy with or without pericardiectomy [4]. Preoperative CT and MRI allow surgical planning [3].
- This patient started antituberculous chemotherapy and is continuing treatment in outpatient care. He is expected to start antiretroviral therapy for HIV soon. No surgical treatment was needed until now.
Take Home Message, Teaching Points
- Tuberculous pericarditis should be considered in all cases of pericarditis without a rapidly self-limited course [1].
Differential Diagnosis List
Tuberculous Pericarditis (definite diagnosis)
Tuberculous pericarditis
Pericardial metastasis (namely from lung cancer)
Pericardial mesothelioma
Final Diagnosis
Tuberculous Pericarditis (definite diagnosis)