Figure 1
Urgent (same day) unenhanced and post contrast multidetector CT

Preliminary unenhanced CT acquisition confirmed physical finding of right groin swelling at surgical site (note metallic clips at the skin), due to extensive oedematous fat stranding with minimal fluid (*). Note contralateral fat-containing inguinal hernia (o).
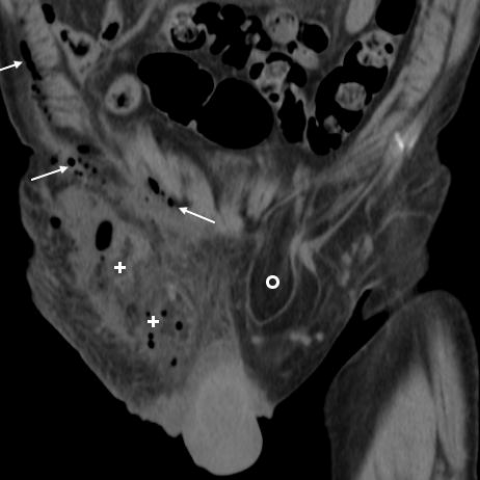
The right groin swelling was mostly occupied by extensive oedematous fat stranding (+) with sparse gas bubbles. Note moderate postsurgical air in the ipsilateral abdominal wall (thin arrows), contralateral fat-containing inguinal hernia (o).

Additionally, mildly obliqued coronal reconstruction showed non-haemorrhagic fluid (15-18 HU attenuation) fluid (*) along the extrainguinal spermatic cord, plus a focal ovoid structure (arrowheads) in the right iliac fossa corresponding to sonographic finding (Fig.1c).

Corresponding oblique-coronal reconstruction after i.v. contrast confirmed focal ovoid structure (arrowheads) abutting the internal inguinal ring, non-haemorrhagic fluid (15-18 HU attenuation) along the extrainguinal spermatic cord (*) without contrast extravasation indicating active bleeding.

Axial post-contrast image after i.v. contrast confirmed groin swelling with oedematous fat stranding, sparse gas bubbles (thin arrow), and fluid (*) along the spermatic cord, without signs of active bleeding.

Axial unenhanced image showed 3.5-cm mass-like structure (arrowheads) in right iliac fossa, with solid periphery and internal fatty attenuation, separated by fat (short arrow) from iliac vessels. Residual abdominal wall air (thin arrow).

Corresponding axial post-contrast image showed nonenhancing 3.5-cm mass-like structure (arrowheads) in right iliac fossa, separated by fat (short arrow) from iliac vessels. Residual abdominal wall air (thin arrow).