Clinical History
A 15-year-old male patient presented with headache and gait disturbance for 1 month. He had no history of convulsion.
Imaging Findings
NCCT brain shows a well-defined hypodense lesion with internal isodense area in the left cerebellar hemisphere (Fig. 1).
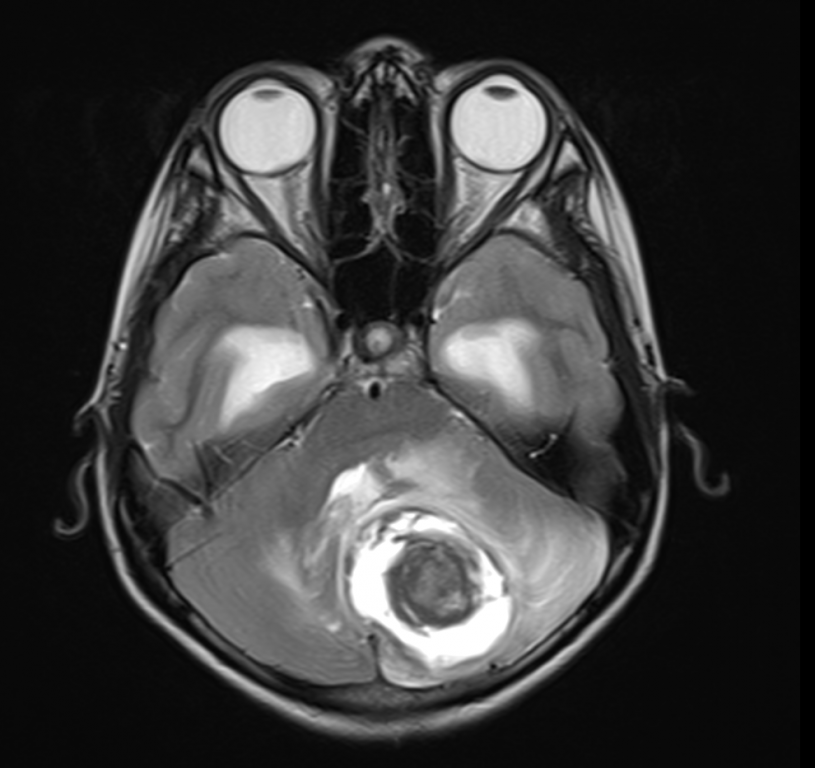
MRI brain shows a well-defined altered signal intensity lesion in left cerebellar hemisphere. The lesion appears hypointense with internal hypo-isointense area on T1 (Fig. 2). On T2W, the lesion appears hyperintense with inner hypointense area. The lesion causes mass effect in the form of compression over 4th ventricle and resultant mild hydrocephalus and periventricular oozing (Fig. 3). On FLAIR, there is mild perilesional oedema (Fig. 4). The lesion does not show diffusion restriction. ADC value of the nodule in the lesion was 1.47 x 10(-3) mm(2)/s. (Fig. 5). On post-contrast T1W, the lesion shows peripheral rim enhancement with mild enhancement of the inner solid component (Figure 6 & 7). The above imaging findings are suggestive of pilocytic astrocytoma.
Biopsy of the lesion showed bipolar cells, rosenthal fibres, multipolar cells and eosinophilic granular bodies.
Discussion
Pilocytic astrocytoma (PA) is a rare, slow-growing glioma, classified as grade I by the WHO [1]. It is the most common paediatric CNS glial neoplasm and the most common paediatric cerebellar tumour. Pilocytic astrocytoma occurs most commonly in children and young adults, with most cases (75%) manifesting in the first 2 decades of life. No gender predilection is reported. Most of the lesions occur in or near midline, usually arising from the cerebellum, the optic nerve and chiasm, or region of the hypothalamus-thalamus. In adults, the tumour more frequently occurs in the cerebral hemisphere. The association of pilocytic astrocytoma with neurofibromatosis type 1 is well documented [2].
The macroscopic appearance of PAs is typically well-circumscribed, cyst-like masses with a discrete mural nodule. The name “pilocytic” is derived from the long, hair-like projections that emanate from the neoplastic astrocytes [1].
Signs and symptoms are usually of several months’ duration and are directly related to the size, location, and presence of associated hydrocephalus. PAs usually follow an indolent course, with an extremely high survival rate [1].
At CT, most pilocytic astrocytomas have a well demarcated appearance with a round or oval shape smaller than 4 cm in size, cyst-like features, smooth margins, and occasional calcifications. Almost all (94%) enhance, typically intensely, on post-contrast images [2]. At MR imaging, pilocytic astrocytoma is typically isointense to hypointense relative to normal brain with T1-weighted sequences and hyperintense with T2-weighted sequences [2]. The appearance of PA on MRI is variable and depends on the tumour’s size and structure. Four predominant imaging patterns: a mass with a non-enhancing cyst and an intensely enhancing mural nodule; a mass with an enhancing cyst wall and an intensely enhancing mural nodule; necrotic mass with central non-enhancing zone; and predominantly solid mass with minimal to no cyst-like component. However, approximately 50% of the tumours are cystic, with a mural nodule attached to one part of the cyst wall [1]. MR spectroscopy performed on the soft-tissue portions have documented elevation in the choline (Cho) to N-acetylaspartate (NAA) ratio, ranging from 1.80 to 3.40. Elevated Cho/creatine (Cr) and lactate/Cr ratios have also been noted, whereas the NAA/Cr ratio has not been significantly elevated [2]. Differential diagnosis includes ependymoma and medulloblastoma. Ependymomas might have calcifications (50 %) and tend to extend laterally to the cerebellopontine angles, while medulloblastomas tend to disseminate through the CSF spaces to the brain and spine [1].
Surgical resection is considered the treatment of choice and is generally regarded as curative when a gross total resection is attained [2].
Differential Diagnosis List
Pilocytic astrocytoma
Medulloblastoma
Haemangioblastoma
Ependymoma
Pleomorphic xanthoastrocytoma