Clinical History
37-year-old male patient presented to ED with 2 weeks of sudden onset mid/low back pain with associated abdominal and testicular discomfort, constipation, erectile dysfunction and lethargy. He has recently been diagnosed with hyperthyroidism and commenced carbimazole but had no other history. Family history included atrial fibrillation and hereditary haemochromatosis.
Imaging Findings
Initial blood tests revealed an obstructive pattern on liver profile.
An abdominal ultrasound was performed to investigate further and revealed incidental complex, septated renal cysts.
The patient underwent Triple Phase Renal CT to further investigate these cysts. A large hyperdense area of thrombus in the infra-renal IVC, extending from the proximal iliac veins to the level of the renal veins, was discovered on CT. There was associated extensive collateralisation and a filling defect of the IVC supra-renally. (Fig. 1a-c)
Discussion
Inferior vena caval atresia or agenesis (IVCA) is a rare condition affecting between 0.0005 - 1% of the general population [1]. It is more commonly seen in young men, with an incidence of up to 5% in patients under 30 presenting with an unprovoked proximal deep vein thrombosis (DVT) [1]. The origin of IVCA is poorly understood, however, it is proposed that it arises from embryonic dysgenesis [2].
There are few reported cases of this condition in the literature. The diagnosis and management of IVCA poses a challenge to medical professionals due to the low incidence, variable presentation, lack of utility of conventional imaging modalities for detection and paucity of established treatment protocols.
Diagnosis, as in this case, is often delayed. Patients may present with any constellation of symptoms secondary to venous congestion including: low back pain, abdominal discomfort, lethargy, testicular pain, erectile dysfunction or symptoms of deep vein thrombosis (especially unprovoked proximal or bilateral DVT) [3]. IVCA can also be associated with congenital biliary atresia or polysplenia syndrome [1].
Imaging modalities such as X-ray and ultrasound are unhelpful in the diagnosis of IVCA. If venous malformation is suspected then MRA or CT with intravenous contrast should be performed [1].
There is no clear consensus as to the best therapeutic strategy for IVCA. Intervention is on a case-by-case basis using novel management strategies without defined treatment guidelines. Treatment options include:
-Conservative management: Thromboembolic deterrent stockings, long-term oral anticoagulation, avoiding precipitants of venous thrombosis such as prolonged immobility [1].
-Interventional Radiological procedures: Pharmacomechanical Catheter-Directed Thrombolysis (PCDT) [4]
-Surgical Intervention: Endovascular intervention such as stenting of collateral venous supplies, atresic veins, stenoses or surgical bypass grafting to relieve venous congestion [2].
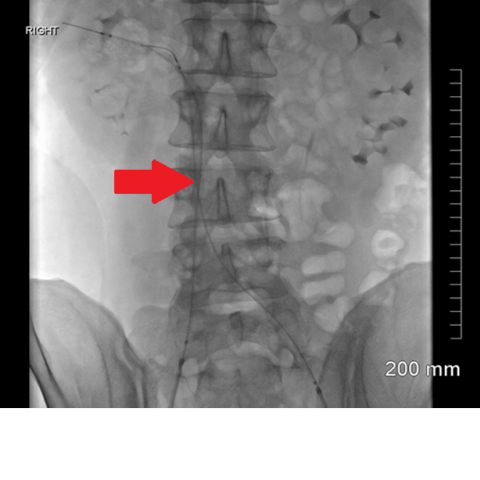
In this case venogram-guided PCDT was performed (Fig. 2a-c) with the aim of:
-Preventing post-thrombotic limb secondary to deep venous valve damage and insufficiency.
-Preventing right renal vein thrombosis and injury.
-Treating symptoms of erectile dysfunction and back pain.
IVCA is seldom encountered in clinical practice and there is currently a lack of long-term data regarding clinical outcomes to guide best practice, therefore early recognition and optimal treatment pose difficulties. The advent of interventional radiology means IVCA is potentially treatable, with the possibility of restoration of normally functioning anatomy. Pioneering interventional techniques and shared international expertise can drive future improvements in the management of this challenging condition.
Differential Diagnosis List
Inferior vena caval thrombosis secondary to supra-renal inferior vena caval atresia or agensis (IVCA)
Intrauterine or perinatal thrombosis of the IVC [5]
Artefactual filling defect of the IVC e.g. pseudothrombosis [6]
Bland thrombosis of the IVC e.g. secondary to a hypercoagulable state [6]
Malignant cause of thrombosis/filling defect [6]
Final Diagnosis
Inferior vena caval thrombosis secondary to supra-renal inferior vena caval atresia or agensis (IVCA)