Figure 1
Non-enhanced MDCT

Volume-rendering reconstruction of the right hand of our patient.
Musculoskeletal system
Case TypeClinical Cases
AuthorsMirko TRENTADUE, MD*; Claudia CASTELLI, MD^; Matteo BRUNELLI, MD, PhD^; Roberto POZZI MUCELLI, MD*
22 years, female
[1] Javdan M, et al. (2012) Fibro-osseous pseudotumor of the digit. Adv Biomed Res 1:31. (PMID: 23210090)
[2] Mak KH, Mak KL. (2001) Fibro-osseous pseudotumours in the finger: a report on their recurrence. Journal of Orthopaedic Surgery 5(2):117-20.
[3] Folpe AL, Inwards CY. (2010) Bone and Soft tissue Pathology. Saunders Elsevier 239-43 p.
[4] Chaudhry IH, et al. (2010) Fibro-osseous pseudotumor of the digit: a clinicopathological study of 17 cases. J Cutan Pathol 37(3):323-9. (PMID: 19678826)
[5] de Silva MV, et al. (2003) Myositis ossificans and fibroosseous pseudotumor of digits: a clinicopathological review of 64 cases with emphasis on diagnostic pitfalls. Int J Surg Pathol 11(3):187-95. (PMID: 12894350)
[6] Dupree WB, et al. (1986) Fibro-osseous pseudotumor of the digits. Cancer 58(9):2103-9. (PMID: 3463398)
[7] Shankman S, et al. (2004) MR imaging of tumors and tumor-like lesions of the upper extremity. Magn Reson Imaging Clin N Am 12(2):349-59. (PMID: 15172390)
[8] Moosavi CA, et al. (2008) Fibroosseous [corrected] pseudotumor of the digit: a clinicopathologic study of 43 new cases. Ann Diagn Pathol 12(1):21-8. (PMID: 18164411)
[9] Hashmi AA, et al. (2014) Fibro-osseous pseudotumor of the digit presenting as an ulcerated lesion: a case report. Int Arch Med 7(1):4. (PMID: 24405807)
[10] Kransdorf MJ, Meis JM. (1993) From the archives of the AFIP. Extraskeletal osseous and cartilaginous tumors of the extremities. Radiographics 13(4):853-84. (PMID: 8356273)
| URL: | https://www.eurorad.org/case/12935 |
| DOI: | 10.1594/EURORAD/CASE.12935 |
| ISSN: | 1563-4086 |
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.

Non-enhanced MDCT
Plain films
Non-enhanced MDCT
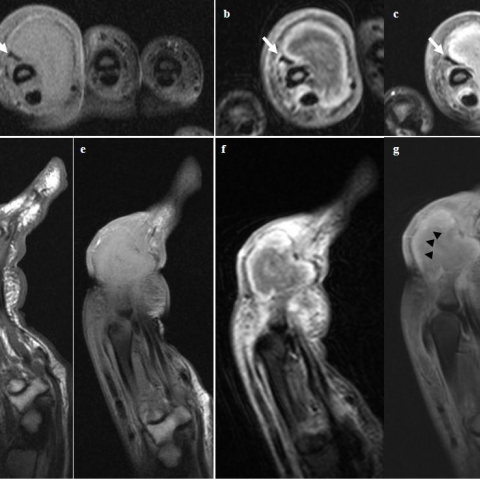
MRI
Histopathological examination
Table 1 - FOPD imaging findings