Figure 1
Pre-procedural contrast-enhanced multidetector CT + percutaneous biliary stenting

Axial (a..c in caudocranial order) and coronal (d,e) images showed solid tissue (arrowheads) corresponding to known carcinoma of the Vaterian ampulla, causing moderate duodenal dilatation (*) and biliary obstruction (+) despite plastic stent in site.

Axial (a..c in caudocranial order) and coronal (d,e) images showed solid tissue (arrowheads) corresponding to known carcinoma of the Vaterian ampulla, causing moderate duodenal dilatation (*) and biliary obstruction (+) despite plastic stent in site.

Axial (a..c in caudocranial order) and coronal (d,e) images showed solid tissue (arrowheads) corresponding to known carcinoma of the Vaterian ampulla, causing moderate duodenal dilatation (*) and biliary obstruction (+) despite plastic stent in site.

Axial (a..c in caudocranial order) and coronal (d,e) images showed solid tissue (arrowheads) corresponding to known carcinoma of the Vaterian ampulla, causing moderate duodenal dilatation (*) and biliary obstruction (+) despite plastic stent in site.

Axial (a..c in caudocranial order) and coronal (d,e) images showed solid tissue (arrowheads) corresponding to known carcinoma of the Vaterian ampulla, causing moderate duodenal dilatation (*) and biliary obstruction (+) despite plastic stent in site.

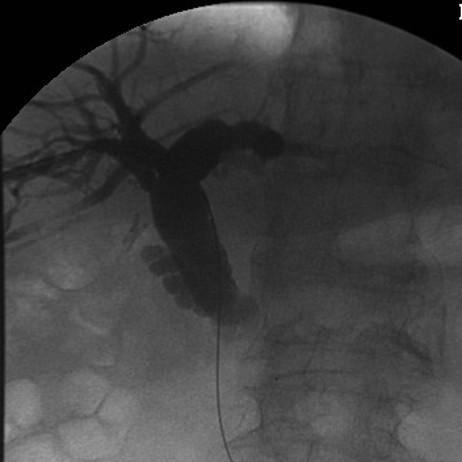
Following removal of plastic biliary stent, percutaneous cholangiographic images showed opacification of dilated intrahepatic and common bile ducts from tight choledochal stricture (f), treated with positioning of metallic biliary prosthesis (g).

Following removal of plastic biliary stent, percutaneous cholangiographic images showed opacification of dilated intrahepatic and common bile ducts from tight choledochal stricture (f), treated with positioning of metallic biliary prosthesis (g).