Clinical History
The clinical examination of a male newborn revealed wide open cranial sutures and fontanelles.
Imaging Findings
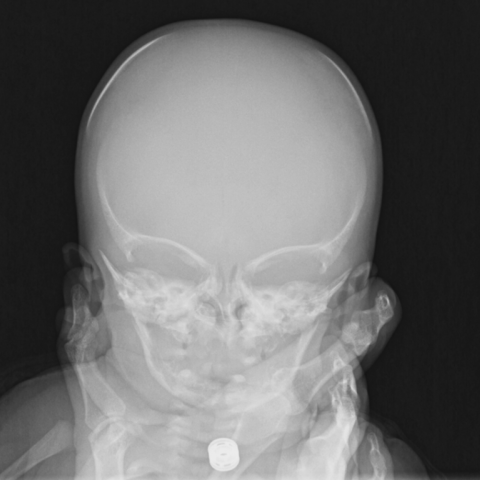
Figure 1 and Figure 2: Frontal (1) and lateral (2) skull radiographs show broad and anomalous cranial sutures with widely patent fontanelles and absent ossification of a portion of the skull bone.
Figure 3: Anteroposterior thoraco-abdominal-pelvic radiograph** reveals hypoplastic clavicles bilaterally, absence of synostosis of the posterior arches of the cervical spine, bilateral shoulder dislocation, diastasis of the pubic symphysis and bilateral dislocation of the hips.
** It should be noted that this type of 'babygram' examination is NOT recommended for the diagnosis of a suspected skeletal dysplasia, rather a skeletal survey examination (only a single view of one upper and one lower limb need be imaged, and a single image of each extremity; the chest, lateral spine, pelvis and skull must also be evaluated) ought to be performed. Section Editor
Discussion
Cleidocranial dysostosis (CCD) is a congenital condition that causes several defects in the bones formed by intramembranous ossification; primarily the clavicles, cranium and pelvis [1]. In 1898, Marie and Sainton, described this disease for the first time [1]. CCD is characterized by abnormalities that affect membranous and endochondral bone [2]. These abnormalities are caused by mutations in the CBFA1 gene, resulting in the production of a transcription factor that activates osteoblastic differentiation (RUNX2) [3, 4].The locus for this dysplasia has been isolated to the short arm of chromosome 6 [4]. Both the dominant and the recessive patterns of inheritance have been described, however, spontaneous mutation occurs in 20-40% of the cases [4].
CCD is a relatively rare congenital defect with a prevalence of 0.5 per 100, 000 live births [4]. Starting from 14 weeks of gestation it is possible to make a prenatal diagnosis using ultrasound [2]. Men and women are affected to an approximately equal extent, and the condition can appear in several successive generations [4]. There are no racial predilections and most patients are of normal intelligence [5].
The clinical presentation of the individuals with CCD is pathognomonic: they usually have short stature, kyphoscoliosis, a large and brachycephalic head [5] with late closure of the sutures and fontanelles [6], small and short face, mandibular prognathism, supernumerary teeth, long and narrow neck, hypermobile shoulders [5], hearing loss [6], cone-shaped thorax with narrow upper thoracic diameter, brachydactyly, tapering fingers and short, broad thumbs [3].
Plain film radiography is the most important imaging modality for diagnosing CCD [4].The skull classically exhibits diffuse areas of rarefaction with most ossification in the frontal bones and the least in the temporal and parietal bones [4], broad and anomalous cranial sutures with patent fontanelles and Wormian bones, underdeveloped paranasal sinuses [4, 5] and lack of pneumatisation of the mastoid air cells [4].The clavicles can appear hypoplastic or aplastic on one or both sides [4, 5].The mandible and maxilla show unerupted and malpositioned supernumerary teeth [4, 5]. The pelvic radiograph can demonstrate a widened pubic symphysis, pelvic dysplasia, small iliac wings, coxa vara, very short femoral necks [1], congenital dislocation of hip and multiple spinal anomalies [4].
There are no specific treatments available for the skull, clavicular or other skeletal abnormalities associated with CCD [5, 7]. Some conventional methods are recommended when musculoskeletal problems are present [7]. Protective headgear can be used whilst the fontanelles remain patent [5]. Aesthetic and functional correction of dentofacial deformities are still being discussed in the literature [4]. Genetic counselling is the most important way to manage the CCD [5]. Usually, carriers of CCD grow well without any significant problems and have relatively normal lives [7].
Differential Diagnosis List
Cleidocranial dysostosis
Pycnodysostosis
Coffin-Siris syndrome
Congenital clavicular pseudarthrosis