Figure 1
Barium swallow oesophagogram

Long, circumferential and symmetric filling defect, smoothly tapering, in the mid third of the oesophagus.
Chest imaging
Case TypeClinical Cases
AuthorsDaniel Ramos Andrade, Célia Antunes, Luís Curvo Semedo, Filipe Caseiro Alves
65 years, male
[1] Kyung Mi Jang, Kyung Soo Lee, Soon Jin Lee, Eun A Kim, Tae Sung Kim, Daehee Han, Young Mog Shim (2002) The Spectrum of Benign Esophageal Lesions: Imaging Findings. Korean J Radiol Jul-Sep; 3(3): 199–210 (PMID: 12271166)
[2] Lewis RB, Mehrotra AK, Rodriguez P, Levine MS (2013) From the Radiologic Pathology Archives: Esophageal Neoplasms: Radiologic-Pathologic Correlation. Radiographics Jul-Aug;33(4):1083-108 (PMID: 23842973)
[3] Mutrie CJ, Donahue DM, Wain JC, Wright CD, Gaissert HA, Grillo HC, Mathisen DJ, Allan JS. (2005) Esophageal leiomyoma: a 40-year experience. Ann Thorac Surg Apr;79(4):1122-5. (PMID: 15797036)
[4] Yang PS, Lee KS, Lee SJ, Kim TS, Choo IW, Shim YM, Kim K, Kim Y. (2001) Esophageal leiomyoma: radiologic findings in 12 patients. Korean J Radiol Jul-Sep;2(3):132-7. (PMID: 11752983)
[5] Karagülle E, Akkaya D, Türk E, Göktürk HS, Yildirim E, Moray G. (2008) Giant leiomyoma of the esophagus: a case report and review of the literature. Turk J Gastroenterol Sep;19(3):180-3. (PMID: 19115154)
| URL: | https://www.eurorad.org/case/11322 |
| DOI: | 10.1594/EURORAD/CASE.11322 |
| ISSN: | 1563-4086 |
Barium swallow oesophagogram
Barium swallow oesophagogram
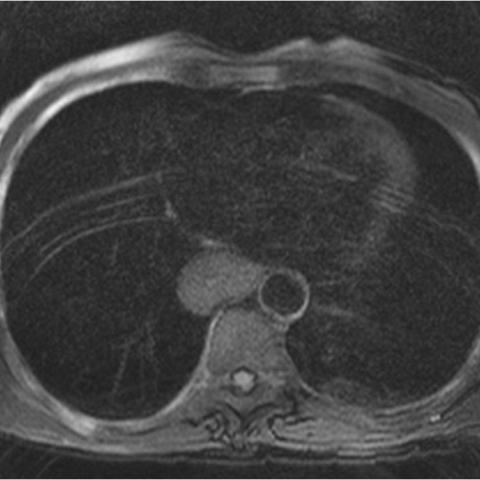
Thoracic MRI - T1w, axial
Thoracic MRI - T1w, axial
Thoracic MRI - T2w FS, axial
Thoracic MRI - HASTE T2w, axial
Thoracic MRI - HASTE T2w, sagittal