Discussion
Commonly known as fibroids, uterine leiomyomas (ULs) are benign proliferations that originate from the myometrial smooth muscle. By far the commonest pelvic tumour in women, ULs are present in more than 20% of women over 30 years of age. Hormone-dependent, ULs are typically encountered during the reproductive age, most frequent in overweight females, may enlarge during pregnancy or oral contraceptive use, and tend to shrink after menopause. Whereas the majority is asymptomatic, ULs can grow to large sizes, sometimes causing palpable masses, heavy menstruation, painful sexual intercourse, or urinary symptoms from bladder compression. Surgical treatment is indicated in cases of bleeding, rapid growth, pelvic pain or pressure symptoms [1, 2].
Pathologically, UL are usually circumscribed, unencapsulated masses, variable-sized and commonly multiple. They represent the commonest cause of uterine enlargement outside pregnancy, and may be either submucosal, intramural, or subserosal. Sudden growth or sarcomatous degeneration (incidence <0.8% of cases) are exceptional [2, 3].
To assess the female reproductive tract, ultrasound is the preferred first-line imaging modality. MRI is increasingly used as a problem-solving tool, particularly for mass characterization, tumour staging and follow-up. Nevertheless, despite ionizing radiation exposure and intravenous contrast use, CT is increasingly performed to investigate acute abdominal and pelvic pain of unknown origin, particularly in emergency settings (when a gynaecologic disorder is not initially suspected, or abnormalities extend beyond the pelvic ultrasound field-of-view) [3-6].
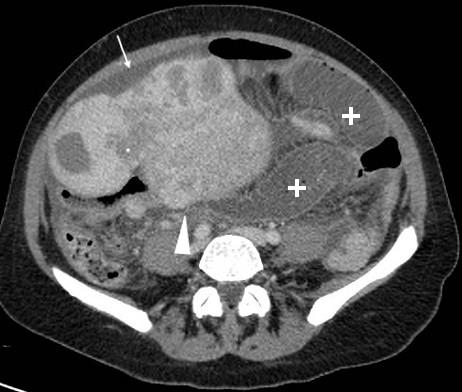
AT CT, uterine leiomyomatosis appears as an enlarged uterus with abnormal, lobulated contours, undetectable endometrial cavity, and presence of solid focal masses with attenuation values similar to those of uninvolved uterus. Variable in location from exophytic or subserosal to intramural to submucosal, ULs show highly variable enhancement, and may thus appear isodense, hypodense, or hyperdense after contrast. Strong hypodensity may result from hyaline degeneration and liquefactive necrosis. Present in only 4% of cases, coarse calcifications are quite specific for UL [2, 3, 5, 6].
Rather rare, giant leiomyomatosis may represent a diagnostic challenge, and requires special surgical considerations. As this case exemplifies, large multilobulated masses with heterogeneous attenuation that protrude from the uterus are compatible with leiomyomatosis, although not diagnostic. Differentiation from malignancies is usually limited, although multiplanar CT reformations help in determining the mass’ uterine origin. Besides increased abdominal girth, leiomyomatosis may cause hydronephrosis, thrombosis from venous compression, and occasionally bowel obstruction. Among the rarest complications associated with leiomyomatosis, the latter results from extrinsic compression by the enlarged uterus and/or adhesions, similarly to pregnancy-related occurrences [1,2,7].