Clinical History
27-year-old Chinese patient was referred for ultrasound evaluation with 6 months history of slowly increasing painless left testicular mass. No other relevant clinical or diagnostic finding could be elicited including lymphadenopathy. Serum alpha feto protein (AFP) & beta human chorionic gonadotrophin (β–HCG) levels were not raised.
Imaging Findings
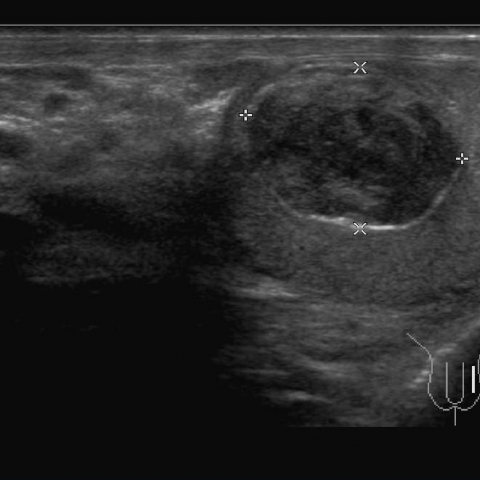
Ultrasound examination revealed a single 1.75 x 1.42 cm sized well circumscribed mass lesion in sub-tunical location of upper pole of the left testis. The lesion was hypo-echoic with concentric ring-like appearance and surrounded by hyper-echoic rim. Colour Doppler showed no appreciable flow inside the lesion with normal flow pattern in rest of the testis. The overall size of left testis was mildly enlarged as compared to the right testis. No evidence of associated hydrocele, varicocele and local or para-aortic lymph-adenopathy could be seen.
Ultrasound features were highly suggestive of benign nature of the mass. Serum α-feto protein & β–HCG levels were well within normal limits. Histopathology sections proved the benign nature of the lesion and ascertained it to be an epidermoid cyst. Patient was offered testis sparing surgery with partial orchidectomy. He recovered un-eventfully.
Discussion
Testicular epidermoid cysts are approximately less than 1% of all testicular masses. These tumours are of epidermal origin, as compared to other germ cell tumours and do not contain hairs or teeth [1]. These are well-circumscribed lesions situated just below the tunica albuginea, having almost completely epithelialised echogenic walls. Epidermoids having internal echoes are clearly differentiated from other cystic lesions. Their whorly appearance, imparted by keratinised contents, gives them characteristic distinction from other intra-testicular lesions. These are usually avascular [2].
The scrotal masses can be classified as: Testicular & extra-testicular.
A) Testicular masses can further be divided into mainly solid – germ cell tumour, stromal cell tumour, lymphoma, leukaemia, metastasis from prostate, lung, melanoma, renal, and GIT, carcinoid, tuberculosis, abscess, inflammatory pseudotumour, haematoma, focal orchitis, sarcoidosis and rare cystic testicular masses – tubular ectasia of the rete testis, cystic dysplasia of the rete testis, non-neoplastic cysts including tunica albuginea cyst, intratesticular cyst, dermoid cyst, epidermoid cyst, benign/mature cystic teratoma, cystic lymphangioma, serous papillary cystic tumour, cystadenoma / adenofibroma of the rete testis, intratesticular spermatocele, intratesticular varicocele, haemorrhage, infarction, and necrosis.
B) The most common extra-testicular scrotal masses are inguinal hernias, though secondary to their inguinal / abdominal origin [3].
Hydroceles are most common extra-testicular masses of scrotal origin [4] Epididymal cysts and varicoceles are other extratesticular masses.
Most of the tumours are diagnosed in third and fourth decade of life [5]. Although, no age is exempt of having scrotal masses. Testicular malignant germ cell tumours constitute 90% to 95% of primary tumours. Germ cell tumours are classified as seminomas and non-seminomatous tumours, with seminomas constituting 40% of germ cell tumours. Mixed embryonal cell tumours and terato-carcinomas are the most common non-seminomatous neoplasms, constituting 25% each of germ cell tumours. Other non-seminomatous neoplasms include yolk sac tumours, chorio-carcinomas, teratomas, and various combinations of these cell types.
Scrotal ultrasound is highly accurate modality for differentiating testicular from extra-testicular masses [6]. It determines whether the mass is cystic, solid, or complex [7]. Extensive understanding of ultrasound features of various scrotal masses clearly defines the nature of these masses in experienced hands. MRI shows high signal intensity in malignant cases but is non-specific and is not routinely used. CT examination is performed for staging purposes [8]. Histopathology augments the final diagnosis and helps decide the surgical options – radical surgery for malignant masses whereas testis sparing surgery in benign intra-testicular masses.
Differential Diagnosis List
Left testicular epidermoid cyst
Malignant testicular mass
Chronic infection
Haematocoele
Haematoma
Final Diagnosis
Left testicular epidermoid cyst